Frozen Shoulder
The frozen shoulder is one of the most painful and debilitating shoulder pathologies one can have. It is a condition with no known cause in the majority of cases, generally with spontaneous onset. It is most common in females (40-60 years age), but does occur in males and other age groups. It may follow injuries, operations, or be associated with medical conditions like diabetes mellitus. It is referred to as “adhesive capsulitis” suggesting that the capsule is inflamed and adhering (clinging) to the joint, causing pain and limitation of motion.
In my experience this is one of the most debilitating conditions one can develop in the shoulder. It can be extremely painful to move the arm away from the body causing at times severe functional limitations. The patient is left scratching their head trying to figure out what happened to cause this. In most cases, there is no clear cause. Progress to the point of resolution can be stubborn and prolonged. Fortunately there are several very effective treatments.
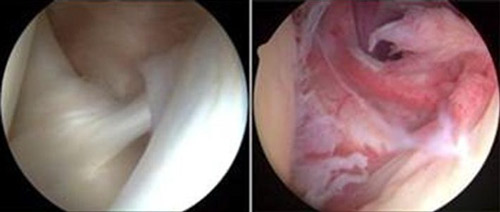
Arthroscopic images of normal capsular tissue and inflamed capsular tissue/
adhesive capsulitis
In a Frozen shoulder, the normal joint lining (capsule) becomes intensely inflamed. This inflammation causes pain at rest but severe pain if you stretch the tissue (i.e. move your arm well away from your side). In the schematic and arthroscopy photos below, you can appreciate the difference between the normal capsular tissue and the inflamed tissue in the same region of shoulders.
This capsular inflammation will eventually lead to scarring of the tissue, and the once relatively thin and normally elastic capsular tissue will become significantly scarred/thickened, and non-elastic. At this stage of the pathology your arm will no longer travel through a full range of motion. The Frozen shoulder is thought to progress through stages as outlined below.
- Stage One: In the "freezing" stage, which may last from six weeks to nine months, the patient slow onset of pain. As the pain worsens, the shoulder motion is lost.
- Stage Two: The "frozen" stage is marked by a slow improvement in pain, but the stiffness/motion restriction remains. This generally lasts four months to nine months.
- Stage Three: The final stage is the "thawing", during which shoulder motion slowly returns towards normal. This generally lasts five months to 26 months.
In most cases, left alone, the process will eventually improve naturally with time. However the process can be long and extremely debilitating and often patients will not recover full motion without treatment.
Treatment
Early recognition is important as patients respond quicker and more predictably to conservative treatments when initiated in the first several months from first symptoms. There are several effective conservative treatment regimens for the treatment of a frozen shoulder. The key elements include anti-inflammation medication and an aggressive stretching program. I have found approximately 80% of the frozen shoulder patients to be effectively treated without the need for surgical intervention. There is a role for over the counter anti inflammation medicine like Advil or Aleve, but in most cases these are not potent enough to eliminate the inflammatory process. I generally recommend an injection of depomedrol (a steroid like cortisone) into the shoulder joint. This provides the most potent anti-inflammatory medicine right at the location of the pathology. Generally the effect is reduced capsular inflammation and reduced shoulder pain so that one can tolerate stretching the shoulder. The stretching is the key. This will ultimately allow restoration of function and resolution of pain. I give patients a home program of self-directed stretches and generally will recommend working with a therapist to more aggressively stretch the shoulder. It is very important to understand that in this situation you must push through the pain in order to get better (Truely: No Pain—No Gain). If recognized and treated early, progress can be rapid, and on other occasions, progress can be tormentingly slow.
For some patients with frozen shoulder, the pain is too great, and the adhesions too rigid, and conservative treatment fails. At this point, I usually recommend progressing to arthroscopic surgery for a capsular release procedure and manipulation under general anesthesia. In this procedure, I use the scope and an electro-cautery blade to selectively release the scarred portions of the capsule. Then a gentle manipulation is performed to restore full fluid motion to the shoulder. This treatment has proven extremely effective and usually yields dramatic and relatively rapid improvement in motion and pain. After this surgery, it is very important to continue daily stretching and therapy to maintain the full motion that I generally achieve during the operation. Recovery generally lasts 4-6 weeks. When conservative treatments fail, I will typically recommend this treatment over the alternative of having the patient simply endure as the disease runs its course.